
Rural Health Transformation Solutions for EMS, MIH and Rural Communities
Supporting the CMS Rural Health Transformation Program
Transforming Rural Health Through Connected, Intelligent Mobile Care
Designed for first responders and care teams who deliver in-home and on-scene care, including paramedics, fire, law enforcement, social services, and community health workers (CHW), HealthCall is the unified platform that state Medicaid policymakers, Departments of Health, Community Risk Reduction leaders, and State EMS officials trust to operationalize and scale care delivery in rural communities as part of a broader rural health transformation effort.
HealthCall is an end-to-end care delivery platform designed specifically for Community Paramedicine and Mobile Integrated Health (CP-MIH), helping programs improve health outcomes while expanding sustainable access through scalable rural health innovations.
Guided workflows support virtual care before and between visits, on-scene documentation with decision support, and follow-up care with remote patient monitoring, backed by the operational and data infrastructure CP-MIH programs need: structured care coordination, consistent documentation and reporting, program oversight and accountability, and readiness for future reimbursement models that strengthen healthcare access.
Supporting the Rural Health Transformation Program
HealthCall operationalizes the rural health transformation program by turning community paramedicine and mobile integrated health (CP-MIH) strategy into a patient-centered, predictable field execution process with system-level visibility. The platform connects referral intake, risk stratification, and clinical workflows with guided documentation, remote monitoring, and closed-loop follow-up, so every encounter is captured consistently and negative trends are identified early, enabling proactive care. Program leaders gain real-time metrics for utilization and compliance across agencies and regions, advancing health transformation with standardized protocols, performance management, and efficient care delivery through technology-driven solutions.
End-to-End Care Delivery Platform for Rural EMS, MIH, and Community Partners
Rural health transformation succeeds when care is repeatable in the field, measurable across agencies, and scalable statewide, without adding burden to crews. HealthCall is an end-to-end care delivery platform that connects virtual care, on-scene clinical execution, and longitudinal follow-up into one guided workflow. It unifies the full episode of care before, during, and after an encounter, so mobile teams can deliver consistent care with system-level oversight.
Built for rural collaboration, HealthCall connects EMS and CP-MIH teams with public health, behavioral health, social services, and community health workers. Programs can standardize protocols across regions while preserving flexibility for local workflows and multidisciplinary partners. The result is more predictable field execution, stronger continuity of care, earlier risk detection, and fewer avoidable escalations, supported by consistent documentation and reporting that strengthens governance and reimbursement readiness. Program leaders gain shared visibility into utilization, compliance, and outcomes, without chasing paperwork.
A Robust Suite of Integrated Services and Guided Workflows
HealthCall differentiates by unifying the full episode of care, before, during, and after each encounter, inside one connected platform.
Virtual care before and between visits:
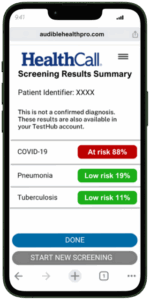
Teams can engage patients earlier through virtual access, screening, and 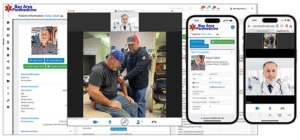 outreach. One-click Telehealth connects crews and clinicians for consults and escalation. AI-powered respiratory and vitals screening surfaces risk signals and guides next steps, while APR Assistant supports symptom checks, adherence, and patient communications between visits.
outreach. One-click Telehealth connects crews and clinicians for consults and escalation. AI-powered respiratory and vitals screening surfaces risk signals and guides next steps, while APR Assistant supports symptom checks, adherence, and patient communications between visits.
On-scene documentation with decision support:
 In the field, HealthCall enables flexible, compliant documentation that supports Treat In Place (TIP) and Triage to Alternate Destination (TAD). Guided workflows reduce variability and help capture the right data the first time. A true longitudinal record and comprehensive EHR capabilities keep history, prior assessments, and care plans available across repeat encounters. SMART Charts and a large assessment library standardize protocol-driven documentation and decision support.
In the field, HealthCall enables flexible, compliant documentation that supports Treat In Place (TIP) and Triage to Alternate Destination (TAD). Guided workflows reduce variability and help capture the right data the first time. A true longitudinal record and comprehensive EHR capabilities keep history, prior assessments, and care plans available across repeat encounters. SMART Charts and a large assessment library standardize protocol-driven documentation and decision support.
Real-time monitoring for Hospital at Home:
HealthCall enables HaH by combining workflow orchestration with continuous remote patient monitoring (RPM). Through the HealthCall Care Network, teams manage enrollment, daily operations, escalation pathways, and interdisciplinary communication in one place. Integrated devices capture and trend vitals (e.g., AliveCor 12-Lead EKG, pulse oximetry, temperature, blood pressure, glucose, and weight), reducing manual charting and enabling earlier intervention. Priusmed streaming vitals plus real-time audio/video supports immediate visual assessment when thresholds trigger concern.
Follow-up care with remote monitoring:
After the encounter, HealthCall closes the loop with RPM, device-free monitoring via APR Assistant, and patient satisfaction surveys; helping detect deterioration early, reinforce care plans, and reduce avoidable ED visits/readmissions.
Operational and Data Infrastructure for CP-MIH Programs
Scaling CP-MIH requires more than a mobile documentation tool; it requires operational infrastructure that connects people, workflows, and performance. HealthCall enables structured care coordination through a secure Community Care Network that supports connected, collaborative care across EMS, clinics, hospitals, public health, and community partners. Real-time updates, task assignment, and shared visibility keep teams aligned on what’s next for each patient, with access across providers to reduce handoff gaps.
HealthCall also drives consistent documentation and reporting through standardized workflows that automate elements of compliance, reimbursement support, and quality reporting, while maintaining HIPAA- and NEMSIS-compliant data capture. Integrated reporting and analytics give program leaders visibility into utilization, outcomes, protocol adherence, and regional variation, supporting program oversight and accountability. Dashboards and alerts help spot gaps early and manage performance at scale. As reimbursement models evolve, HealthCall provides the documentation consistency, audit readiness, and governance capabilities needed to demonstrate value and sustain rural access.
Start Your Rural Health Transformation Initiative
Talk with a specialist about implementing scalable, technology-driven solutions that improve health outcomes, expand healthcare access, and support sustainable transformation in rural communities.
Frequently Asked Questions
What is the CMS Rural Health Transformation Program and how large is the funding?
The CMS Rural Health Transformation Program is a national implementation effort with $50 billion in total funding. CMS has announced awards to all 50 states, with first-year awards in 2026 averaging approximately $200 million and ranging from $147 million to $281 million. The program allocates $10 billion per year from FY 2026 through FY 2030, with half distributed equally among approved states and half based on factors such as rurality, state policy actions, and the strength of proposed initiatives.
What is the Rural Health Transformation Program and what does it require from participants?
The Rural Health Transformation (RHT) Program is an outcomes-based accountability model administered by CMS. It requires states and implementation partners to define performance measures, identify measurable outcomes, report progress annually, and support those reports with reliable data. Programs must provide quantifiable metrics, baseline data, targets where possible, and at least one metric showing impact at a county or community level.
Is RHT funding guaranteed once a state receives an award?
No. RHT funding is conditional and tied to measurable progress. CMS uses a checkpoint model to assess whether states are meeting milestones, policy commitments, and performance targets. Future budget periods can increase or decrease based on a state’s documented progress. CMS can also recover funds previously awarded if a state fails to fulfill a policy commitment by the required deadline. This makes reporting infrastructure a core part of the program, not an afterthought.
What happens if a state does not meet its policy commitments under RHT?
According to the NOFO, if a state policy commitment is not fulfilled by the required deadline, the points associated with that commitment will decrease to zero and CMS will recover funds previously awarded based on that factor. This means states and their implementation partners face real financial risk if documented progress does not match the commitments that supported the original award.
What performance measures does CMS expect RHT programs to track?
CMS requires quantifiable metrics, baseline data, targets where possible, identified data sources, and annual performance metric progress reporting. CMS examples include access metrics, readmission rates, chronic disease rates, opioid overdose death rates, financial stability indicators, workforce metrics, telehealth access, interoperability scores, and program implementation measures. At least one metric must demonstrate impact at a county or community level.
What is the difference between outcome measures and lead measures?
Outcome measures show whether a program is producing its intended result, such as reductions in emergency department visits, hospital admissions, or chronic disease complications. Lead measures show whether the work required to achieve those results is actually happening, such as referrals received, patients enrolled, home visits completed, care plans updated, and follow-ups closed on time. Both are important because many RHT outcomes take time to materialize.
Why are lead measures important if the goal is to demonstrate long-term outcomes?
Long-term outcomes such as reduced emergency department utilization, lower readmission rates, and improved chronic disease control take time to validate. Lead measures allow programs to show that the necessary work is happening now, including referrals received, patients enrolled, encounters completed, follow-ups closed, protocols followed, care plans updated, and patient satisfaction captured. These measures do not replace outcomes but make outcomes more achievable and defensible during compliance reviews.
Does the RHT reporting burden apply only to states, or does it extend to local partners?
The reporting burden extends beyond state government. The NOFO allows states to subaward or subcontract RHT funds to partners such as universities, local health departments, provider associations, and other organizations. Federal award terms and conditions generally flow down to subawards and subrecipients. In practice, EMS agencies, MIH programs, hospitals, clinics, public health departments, behavioral health partners, and community-based organizations may all need to document their contribution to a state’s RHT goals.
What is the practical framework for building a successful RHT program?
Successful RHT programs should follow five key principles. First, start with the outcome by defining the baseline, target, time-frame, geography, and data source before implementation begins. Second, map every workflow to a measure so that visits, referrals, assessments, and outreach efforts are documented in a reportable way. Third, manage lead measures continuously rather than waiting for annual reporting to discover performance gaps. Fourth, standardize what must be standardized to give state leaders comparable data while preserving local flexibility. Fifth, prepare for audit and evidence review by keeping milestones, metrics, baselines, and targets traceable and defensible.
Why is Mobile Integrated Health a strong fit for RHT priorities?
Mobile Integrated Health aligns closely with RHT priorities because it brings preventive care, chronic disease support, behavioral health coordination, care navigation, telehealth, and follow-up directly into homes and communities. MIH uses existing EMS and community resources, reduces transportation barriers, supports treatment in place as an alternative to transport, and generates measurable data around utilization and outcomes, all of which are central to what RHT programs are expected to demonstrate.